As can be seen from the above, the sudden drastic increase in the number of infected people can lead to a breakdown in the medical care system, even in large urban areas where there are high medical standards and a high degree of capacity. This, in turn, can lead to high-risk patients being overlooked and an unnecessary increase in infections, which then leads to higher mortality rates.
Thus, we turn our attention to what can be done to prevent the high mortality rate seen in Wuhan from occurring in places like Tokyo and Osaka. The key is preventing widespread infection, which in turn would prevent a breakdown of the medical care system. To achieve this, it is essential that physical contact between people be reduced.
Therefore, on January 23, the Chinese authorities sealed off Wuhan, prohibited all air, rail, and overland travel into and out of the city, and stopped subways, buses, and all other forms of public transportation within the city. These measures were intended to prevent people infected with COVID-19 disease from leaving Wuhan while at the same time preventing people in Wuhan from having physical contact with one another.
The failure to close off the city in time due to the delayed initial response has been criticized. Wuhan mayor Zhou Xianwang made the following statement at a press conference held on January 26: “Due to the Spring Holiday [the New Year's holiday in China] and the novel pneumonia outbreak, at present over 5 million people have left Wuhan.” It cannot be ruled out that this was one cause of the spread of the infection across the world.
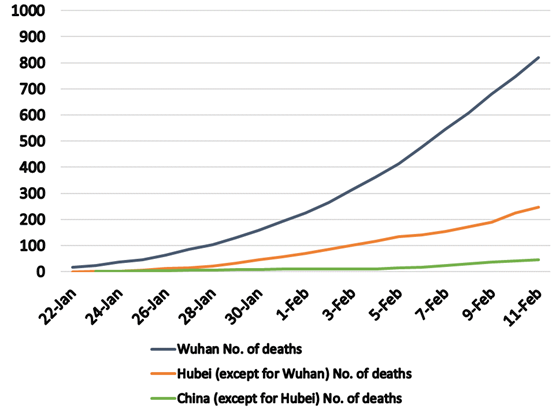
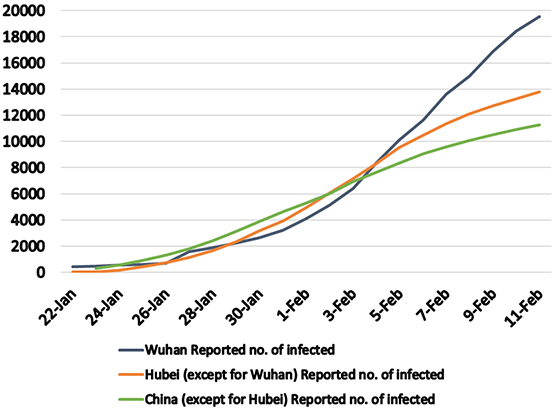
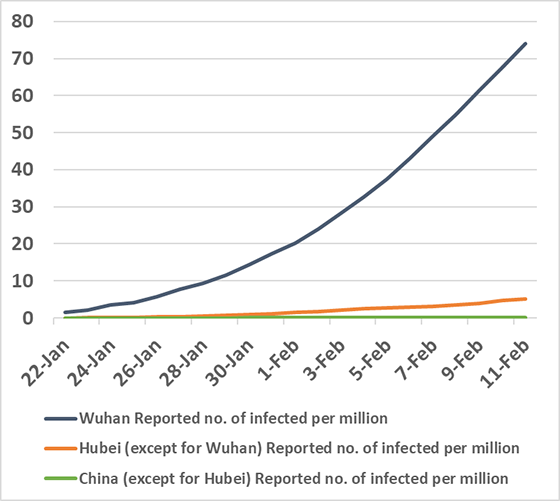
However, as can be seen from the three figures discussed above, despite the fact that the lockdown of the city of Wuhan was delayed, it is also true that this action prevented the breakdown of the medical care system in other regions of China, and it mitigated increases in the numbers of deaths in other regions of China. In addition, Wuhan itself—where internal movements were restricted—was successful in mitigating increases in the number of newly infected people.
A state of emergency was declared in Japan on April 7 to prevent a vast outbreak of infection and the breakdown of the medical care system. At the start of a press conference held that same night, Prime Minister Abe Shinzo thanked healthcare professionals and stated, “We will do everything necessary to protect locations where medical care is being provided.” Thus, he clearly indicated that the purpose of the emergency declaration was to prevent a breakdown of the medical care system.
The prime minister has been criticized for taking this action too late. However, if even in China, where people have pointed out the failures that resulted from these same kinds of delays in initial action, the lockdown of cities and the expansion of the medical care system facilitated the prevention of breakdowns in the medical system and mitigated increases in the number of deaths, then this is encouraging news for Japan.
If actual human contact can be reduced in Japan by 70% or 80%, then increases in the numbers of deaths in Tokyo and Osaka due to a breakdown in the medical care system in those cities and more widespread infections in other domestic population centers can be avoided, which will prevent the circumstances that existed in Wuhan from occurring in Japan. The success of such measures, however, depends upon each person's actions.
(Dated Apr 9, 2020)